I
recently came across a young patient with unexplained hyperlactatemia. He came
in with severe abdominal pain and was found to have a normal CT Abdomen with a background of ethanol related chronic pancreatitis . He was
eventually admitted for pain relief and unexplained hyperlactatemia. So I went
back and did a bit of reading on LACTATE...
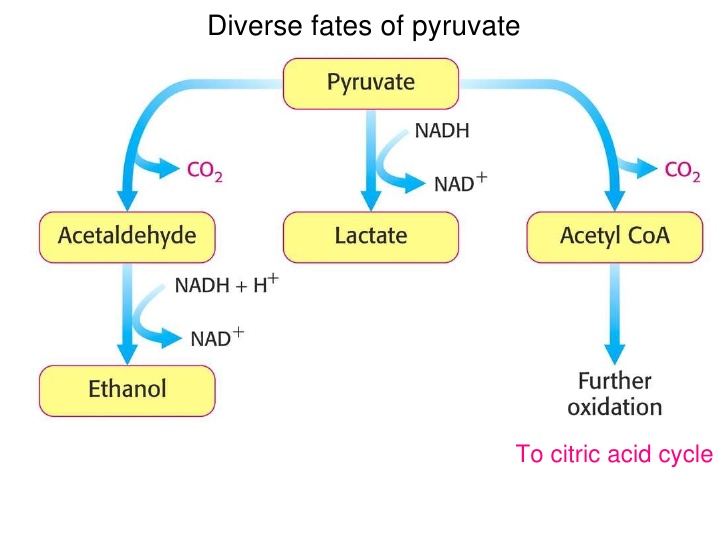
What is Lactate?
Lactate is
the normal endpoint of the anaerobic breakdown of glucose. Most of the lactate production occurs in skeletal muscle,
bowel, brain, and RBCs. The lactate generated can be taken up by the liver and
converted to glucose (via gluconeogenesis) or can be used as a primary
oxidative fuel. In the setting of decreased tissue oxygenation, lactic
acid is produced as the anaerobic cycle is utilized for energy production.
Evidence
suggests increased morbidity and mortality for patients with increasing
lactate levels or a decreased rate of lactate clearance.
How is lactate cleared from our body?
Lactate is cleared from blood by thru liver, kidneys (10-20%) and skeletal muscles. The ability of the liver to consume lactate is concentration-dependent and progressively decreases as the level of blood lactate increases.
Lactate producers: skeletal muscle, the brain, the gut, and the erythrocytes.
Lactate metabolizers: Liver, the kidneys, and the heart.
Lactate v/s Lactic Acid and
Hyperlactatemia v/s Lactic Acidosis.
Lactate
is not synonymous with lactic acid, and hyperlactatemia is not synonymous
with lactic acidosis.
Hyperlactatemia is defined as a persistent, mild to
moderate (upto 4-5 mmol/L) increase in blood lactate concentration without metabolic acidosis. It can occur in the
setting of adequate tissue perfusion, intact buffering systems, and adequate
tissue oxygenation.
Lactic acidosis is characterized by persistently increased
blood lactate levels (usually >5 mmol/L) in association with metabolic
acidosis. Also, lactic acidosis may not
necessarily produce acidemia in a patient. The development of lactic
acidosis depends on the magnitude of hyperlactatemia, the buffering capacity of
the body, and the coexistence of other conditions that produce tachypnea and
alkalosis (eg, liver disease, sepsis). Thus,
hyperlactatemia or lactic acidosis may be associated with acidemia, a normal
pH, or alkalemia.
D-Lactate
and L-lactate
L-lactate and D-lactate are the two isomeric
forms of lactate.
L-lactate is the most commonly measured
level, as it is the only form produced in human metabolism.
D-lactate is
a byproduct of bacterial metabolism and may accumulate in patients with
short-gut syndrome or in those with a history of gastric bypass or small-bowel
resection
What causes an elevated lactate?
- Tissue
Hypoxia and Anaerobic Metabolism (Traditional school of thought)
- Due to
decreased clearance rather than increased production in sepsis
- Secondary
to down-regulating of pyruvate dehydrogenase in skeletal muscles by
inflammatory mediators (Cytokines) and Catecholamines.
Is it possible to have hypoperfusion but a
normal lactate level?
Short
Answer- YES
For
significant increase in blood lactate to occur, lactate must be released into
the systemic circulation and the rate of production must exceed hepatic, renal,
and skeletal muscle uptake. Therefore, regional hypoperfusion of tissues may be
present despite normal blood lactate concentrations.
Types of Lactic Acidosis
- Type A – Poor tissue perfusion or
oxygenation of blood (eg, hypotension, cyanosis, cool and mottled extremities).
It can be caused by the overproduction of lactate or the underutilization of
lactate. For instance, muscular activity, seizures, ischemia, shock, hypoxemia,
anemia, CO poisoning.
- Type B - no clinical evidence of poor tissue
perfusion or oxygenation exists.
- Type B1 occurs in association with systemic
disease, such as renal and hepatic failure, diabetes and malignancy, thiamine deficiency,
infection, pancreatitis, short bowel syndrome.
- Type B2 is caused by several classes of
drugs and toxins, including biguanides, alcohols, iron, isoniazid, zidovudine,
and salicylates.
- Type B3 is
due to inborn errors of metabolism.
List of Possible Causes
- Sepsis
related Hypoperfusion and Mitochondrial Dysfunction
- Bowel
ischemia
- Severe
iron-deficiency anemia, Diabetes mellitus
- Liver
disease, Kidney Disease
- Alcoholic
Ketoacidosis, Pancreatitis
- Malignancy
(leukemia, lymphoma, lung cancer)
- Seizures
- Heat
stroke, Pheochromocytoma
- Thiamine
deficiency (Remember this one during ICU rounds!)
- Inborn errors of metabolism - von Gierke disease,
fructose-1,6-diphosphatase deficiency, pyruvate carboxylase deficiency,
pyruvate dehydrogenase deficiency, oxidative phosphorylation deficiency, and
methylmalonic aciduria.
- MELAS syndrome (mitochondrial encephalopathy, lactic
acidosis, and stroke like episodes) - Characterized by migraine like headaches,
dementia, hearing loss, ataxia, and episodic vomiting
What drugs can cause an elevated lactate?
•
Acetaminophen
•
Alcohols
and glycols (ethanol, ethylene glycol, methanol, propylene glycol)
•
Antiretroviral
nucleoside analogs (zidovudine, didanosine, lamivudine)
•
Beta-adrenergic
agents (epinephrine, ritodrine, terbutaline, salbutamol)
•
Biguanides
(phenformin, metformin)
•
Cocaine
•
Cyanogenic
compounds (cyanide, nitroprusside)
•
5-FU
•
Iron, Isoniazid
•
Propofol
•
Salicylates
•
Sulfasalazine
•
Valproic
acid
Click here to listen to Scott Weingart talking about Lactate
Take Home:
- Get familiar with Type B causes of an elevated lactate
- See the medication list and co-morbities while evaluating elevated lactate
Other Resources:
EMCrit/Pulmcrit on Lactate
Resus.me
Author:
Lakshay Chanana
Speciality Doctor
Northwick Park Hospital
Department of Emergency Medicine
England