As Emergency Medicine is a new specialty and
there has been a lot of buzz around it, if you are a medical graduate in India
wanting to take up Emergency medicine you would definitely be perplexed by the
myriad of nomenclatures of EM postgraduate qualifications. As an MBBS pass out
when you are vaguely starting to understand what different specialties are and
what EM is, just when you think you might have a thing for EM, you probably are
bombarded with countless names (of qualifications), each claiming to be
superior to one another. Everyone seems to have an opinion about EM (like
everything else) - One with a qualification in EM, one without, a doctor who
has no idea what emergency medicine is, that homeopath on the crossroad,
EVERYONE! Just yesterday when I was walking down the road I even overheard the
samosa guy explain to the chaiwala (No no..not Modi!) how one course is better
than the other while he unknowingly obstructed an Ambulance passing by with his
cart although the ambulance had it's sirens and lights on !!!
So what's this confusion about ? And how does a
MBBS student or aspiring EM physician analyze this and make an informed
decision and decide what course to join ? Whom to trust when people are
claiming everything like popular news channels - "First on EM tv",
"You saw it first on nautanki now", "We are the undisputed
No.1" and "Exclusive" ?!
So let me just try to dissect each of the popular
EM qualifications in India. I will try to list the advantages, drawbacks of
each of them. I will try to be as unbiased as possible and try to touch upon
some facts pertaining to recent controversies step by step.

1. MD Emergency
Medicine:
Like all other MD qualifications, this degree is
given by Medical Council of India. Course is run in many medical colleges
across India. There are fixed number of seats.
Q:
What are the advantages:
- Needless to say it is recognized by MCI as it
is run by MCI (kind of dumb point ;-P Filling up the answer sheet will fetch me
some extra marks isn't it? Anyway!)
- You can be a faculty in medical colleges and
hospitals running DNB after the completion of the course.
- Getting a job after MD shouldn't be a problem
at all as MD is a brand in itself irrespective of how good you are.
- Like any other MD final exam, passing is
probably not very difficult (well, I don't have a first hand knowledge here but
I haven't heard of someone flunking the MD final exams multiple times
nevertheless)
- Entry is through NEET. So you definitely have
to work hard to earn a seat** (conditions apply)
- You can write MRCEM exam and DNB exam while you
are at it! So can be a triple degree holder (if you are a degree fanatic) at
the end of your course! (Will explain MRCEM in a bit if you do not know what
that is or confused about it)
- On a lighter
note you don't have to explain your degree to relatives unlike most other
degrees. (Although there's no escaping from explaining what EM is!)
Q:
Wow!!! Then is this the perfect, irrefutable, most 'legitimate' EM degrees of
all ???
A: Hold on. The answer might not be an absolute
no or a blanket yes. There are downsides of course!
- There are many medical colleges where the
department of EM is not completely established or to put it in another way
there's no concept of emergency medicine. The primary faculty for teaching are
not from EM.
Although it can be argued that the origin of EM
roots back to surgical specialties and different skills required for an
emergency physician can be taught by different specialties, the lack of primary
teaching faculty from EM would definitely hamper the 'EM-culture'. While an
anesthetist can be a great teacher of airway skills, an orthopod can teach
reducing a shoulder like none other, none of them can teach the 'EM-mindset'
like an emergency physician, which is the heart of practicing as an emergency
medicine doctor. (Enough, I think I did
too much talking there!)
-**Varmaji's beta
worked hard, passed MBBS with distinction, studied again, got good rank in
NEET, was an adrenaline junkie who wanted to bring a change in people's lives,
was interested in EM, got a MD EM seat in a reputed medical college. Passed
with flying colors. Well done.
LEGITIMATE!
Sharmaji's beta passed MBBS after Salman
threatened him that he will get married before he passes. He once tried to
memorize the full form of NEET but then he felt that was completely
unnecessary. He thought he would do MD EM because someone said he didn't have
to admit patients under him if he did that. He was rich, Sharmaji owned 2 BMWs,
he spilled 1.5 crores and BOUGHT a MD EM seat in the same college as Varmaji's
beta like you buy a kilo of brinjal (Baingan - I can't kill the Hyderabadi in
me) from the market. He also somehow passed. Sharmaji's beta is also MD
Emergency Medicine now! LOL! Legitimacy!? LOLOLOL!
--> So, on a serious note, I'm not saying that
MD EM is all bad. Neither it's sacred and the BEST just because it is run by
MCI. Making blanket statements won't help!
So the bottom-line is - Good score
in NEET --> Good college with good EM dept. with preferably faculty from EM
--> MD EM --> Good.
2. DNB Emergency
Medicine:
Run by NBE (National Board of Examinations)
across different hospitals and some medical colleges across India. Like MD,
they have fixed number of seats.
Q:
What are the advantages:
- Recognized by MCI.
- Can be faculty in medical colleges (There has
always been some controversy regarding DNB candidates being asked for some
additional experience to work as assistant prof in medical colleges, I'm unsure
of the present status) and DNB institutes.
- Entry is via NEET.
- Main factor which might increase the
'LEGITIMACY index' of DNB is that there are no 'management seats'. That means
no one can 'buy' DNB seats. You will have to earn them! That's commendable.
- Again getting a job shouldn't be a problem. DNB
programs are well known for churning out good doctors historically.
- Final exams are not easy as MD is the general
perception. Which is kind of good. When you pass, people know you deserve it.
- You can of course write MRCEM exams while you
are at it!
Q:
Well, then there are no downsides? That's amazing, isn't it?
A: Nothing is completely blot free! Again some
downsides are:
- This one is common: Some hospitals might not
have primary faculty from EM.
- Secondary DNB eligibility: Dude, this is a
JOKE! Anyone with ANY diploma is eligible for secondary DNB EM. Like Dip
microbiology, pathology etc. can take up DNB EM (secondary). What on the earth
were they thinking while they made these criteria?! What are they trying to
do/achieve ?! Bizarre!
Bottom-line: Good hospital --> DNB EM --> Very Good.
3. MRCEM (UK):
Membership of Royal College of Emergency Medicine, United Kingdom.
There has been lot of confusion regarding this.
So let's make few facts clear.
1. This is NOT an Indian qualification. This is
awarded by RCEM, UK.
2. It is recognized by MCI as an additional
postgraduate qualification and can be added to your certificate in state
medical councils (I personally know many people who have registered their
qualifications)
3. You can apply for faculty positions in medical
colleges with MRCEM as per the latest notification by MCI. You can find it
here: https://www.mciindia.org/documents/e_Gazette_Amendments/TEQ-11.03.2017.pdf
(I don't have first hand info about anyone who
have done so yet - So unsure of the process involved)
4. You can get job in any hospital after MRCEM
easily.
5. You are eligible for working in UK/Ireland
and/or undergo higher specialty training in UK towards FRCEM. (You are exempted
from PLAB). FRCEM is recognized in Australia as well.
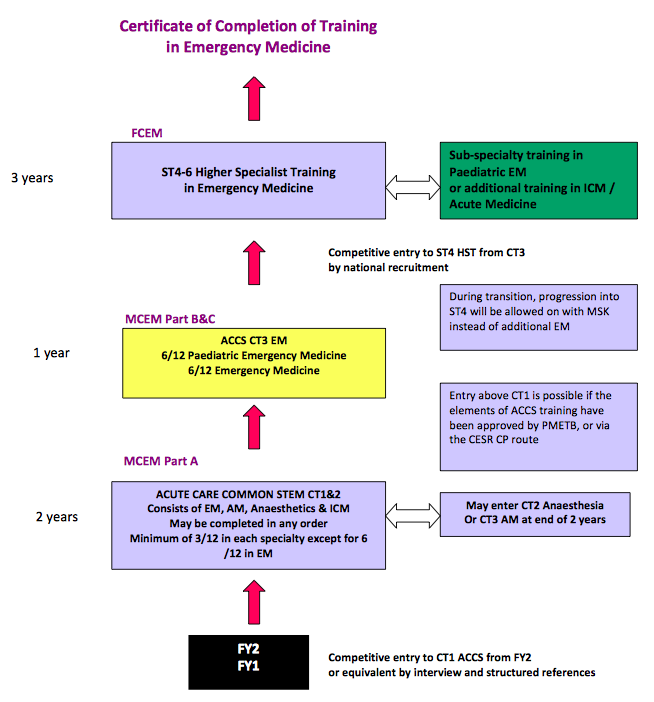
Note : With MRCEM in your pocket, you are eligible to work as a Registrar in UK, NOT as a consultant. However, in India - you will be offered consultant posts by many hospitals after you pass MRCEM exams. MRCEM is half way through training. Emergency Medicine training lasts for 6 years in UK and FRCEM is required before you start working as a consultant. Here is UK training pathway in Emergency Medicine:
6. Do you have to be in a specific
residency or training program to attempt MRCEM exam? The answer is NO. You need to have the evidence of structured
training/experience in EM and allied specialties as per RCEM requirements -
Emergency medicine, Intensive Care medicine, Anesthesia, Acute/Internal
medicine (For roughly 3 years) and you can attempt the exam.
Follow the RCEM link for minute details of exams
and everything else: http://www.rcem.ac.uk/
7. Is the exam easy? Hell no! You would know this if you speak to the
people who have either passed or attempted the exam. Also if you look at the
pass percentage of the exam you will have a fair idea how difficult the exam
is. The pass percentage in each part is
roughly around 25-30. (The exam has 3 parts - A, B, C - Recently changed to
FRCEM primary, intermediate and OSCE - Will not get into the details and add to
the confusion - Refer website for finer details)
8. What's the Apollo connection
with MRCEM ?
This has always been a longstanding doubt of
many. Simple. Apollo was the first in the country to collaborate with RCEM and
start the MRCEM exams in India and started a structured training program in EM
providing training to pass MRCEM back in 2005 (During a time when EM was not
even a MCI recognized specialty in India), pioneering the development of EM in
India.
Apollo runs a structured 3 year EM residency
program training you for MRCEM.
So MRCEM exams are usually held at Apollo
hospitals. Recently there have been few other centers like Max Hospitals, Delhi.
9. So is it mandatory to get
training in Apollo to be eligible for MRCEM ?
No. Absolutely not. College (RCEM) doesn't mind
where you do your training from as long as you are competent and can show the
evidence of same neither they RECOMMEND any specific training program.
So basically you can write MRCEM after MRCEM residency
in Apollo, DNB EM, MD EM, MEM, or not enrolling yourself into any of the
courses per se and just gaining the necessary experience/training in the
specialties mentioned above.
10. So is doing residency in Apollo
useless if my aim is doing MRCEM ?
Definitely not! They have a very good EM dept.
where there are seniors/registrars/consultants who have completed MRCEM who can
guide you. It's a JCI accredited hospital and you have defined protocols. You
have a decent patient load and fair amount of independence. You are rotated
through different specialties ALMOST as per the RCEM curriculum. They can train
you before the exam. Having expert guidance is the key to pass MRCEM apart from
having good training and experience. + The EM culture in Apollo is good and you
will have your identity as an emergency physician. (This is only with Hyderabad
where I worked and Chennai where I have few of my friends - I can't comment
about other Apollo Centres)
Having said that just because you have enrolled
for the residency program doesn't automatically mean that you will pass MRCEM
exam. You are not joining a 'course' where you will be spoon-fed. You will have
to earn it!
11. Can I join any other hospital,
college without enrolling into a course/training program and still clear exam ?
Well, nothing is impossible. You CAN do that as
well provided you have a very good guide and you exactly know what you are
doing. There are people who have done that as well. So it is completely up to
you! Thinking out of the box is a core quality of an emergency physician! But
you have to judge how much out of the box!
12. What in UK after MRCEM ?
Most of the UK training programs run for 6 years
(ST1 - ST6). So you will be entering as a middle grade registrar (ST3/4 level)
after MRCEM. You can complete rest of the years in UK and can also apply for
subspecialty training in Pediatric EM and Prehospital EM. You can also opt for
dual accreditation in ICM which is for 6 years post MRCEM (FFICM). (Again, not
getting into the different pathways after MRCEM for higher specialty training -
Refer to college website for the same)
Downsides:
- Some of the corporate hospitals with training
programs for MRCEM pay very (very) less! (So you will be devoid of money for 3
years and the restaurant owner will be singing 'Abhi na jao chodkar ye bill
abhi bhara nahi'). Some of the hospitals do not pay residents for first 6-8
months of training (Zero – Yeah! You will be doing some charity work for the
poor and needy corporate hospitals.....Smirk, smirk!)
-No leaves for the entire 3 year (almost 1100 days) duration except
for the post night offs. (Note that this is a common problem with most courses
and not specific to this)
- Training can become dull/not-so-happening
sometimes especially if there's shortage of staff.
-The place you choose for training is extremely
important. Especially if it is not a structured training program – High chances
of losing focus, getting lost and getting discouraged by ill informed peers,
colleagues and 'experts' from other specialties.
-There are only a handful of MRCEM qualified
doctors in India. Choosing the right guide in a right hospital out of a
training program might be a tedious task.
Bottom-line: You need to find a very good hospital and have adequate training/experience
to clear MRCEM. A good guide/team is equally important. Exam is definitely not
easy. You will have to earn this qualification. Scope: Very good! MRCEM opens
up many doors for work/training in India and abroad.
PS: One other major downside would be explaining
MRCEM to everyone after you are half dead explaining what emergency medicine
is. Whenever that new uncle goes
"Beta, kya kar rahe ho aajkal?" You will be like 'Maar daalo
mujhe...Maar do!'
4. MEM
(Masters in Emergency Medicine):
MEM (Masters in Emergency Medicine) is a three
year course run by 2 societies - George Washington University, USA and SEMI -
Society for Emergency Medicine, India. Probably this is the most
'controversial' of them all.
Before I start, I'm making it clear that I'm not
jumping into the argument of whether or not these societies can give masters
degree , universities act, it's just a certificate, should it be called
something else etc. Etc. - I'm not a legal expert. Period. Now that these
courses are being run and people have enrolled into them let's see how can they
be assessed by a trainees perspective.
The overview of MEM programs:
1. Are they recognized by MCI ?
A: An absolute NO.
2. Is the GW MEM recognized in USA?
A: No again. A big NO.
3. Is it recognized in UK?
A: NO man, NO! Nooooo!
4. Can you get a job after MEM ?
For now, of course you can get a job with fairly
good pay as there's a shortage of doctors to man the EDs. But future is
unclear.
5. Can i write MRCEM after MEM ?
Yes. Of course you can, like anyone else with
similar experience. But your MEM tag has nothing to do with MRCEM exam!
6. So is MEM completely useless ?
Well, No! Again it's unfair to give such a
blanket statement. MEM programs have a good curriculum (Although not all the
centers adhere to it or have a notable training program). There are quite a few
centers running MEM programs with very good training which produce very good EM
physicians and also high success rate in MRCEM. (Example: MIMS Calicut, KDAH
Mumbai, MaxCure Hospitals Hyderabad. There may be other hospitals which have good
training programs and these are just examples of hospitals I'm aware of which
have good training as per few friends and colleagues who had worked there).
Many of the courses conduct regular
classes/academic sessions, some even with overseas faculty.
7. So are MEM trained doctors are
all incompetent ?
No. 'Unaccredited program does not equal to
incompetent trainees' and vice versa (I hate blanket statements, please
clinically correlate - Also remember Sharmaji's son's story)
Downsides:
- Fee for most of GW MEM courses are high.
- Although the training in some hospitals is
good, ultimately everything boils down to success rate in MRCEM! So the
importance of MEM as a standalone qualification is minuscule especially with
it's 'Unrecognized' status.
- Many hospitals use MEM as a way to get cheap
labor - To prevent understaffing of their EDs and ICUs without actually
training them and also underpaying them - Which definitely is a major concern.
- Many people opt for it because they are not
able to get into anything else. (Ease of entry). Which again is detrimental to
the specialty.
- Most of the MEM programs are advertised saying
they are eligible to write MRCEM after MEM which is of course true but what is
the role of MEM per se needs to be seen. Only time can tell the answer ?!
Bottom-line: Joining MEM might not be a very bad
idea if you like the training in a particular hospital running MEM course and
IF THEY ALSO (ACTUALLY) TRAIN YOU FOR MRCEM.
'Only MEM' is probably like a Limbo in Inception!
You are nowhere! (At least in the present scenario)
Few words
about the nomenclature war:
The cause for this confusion is complex. It may
range from personal interests to governmental insufficiency in uprooting the
corruption in the system + the mismatch between supply and demand and
everything in between – Corporate greed, personal agenda, petty politics, lack
of manpower, funding, infrastructure and the extremely complex system of Indian
healthcare. Frankly I don't have one answer for this neither can I think of one
single solution for this. But definitely conflict and 'rational thinking loss'
are detrimental to the growth of EM as a specialty!
There has been a lot of buzz in the social media
after few reports were published in prominent newspapers about EM
qualifications in India. The newspaper articles although highlighted few
problems, it failed to make an unbiased approach and made it appear as if
everything is right with the MD and DNB courses and everything else is wrong
with the other courses. Many polarized opinions were being circulated with
everyone claiming how certain degrees/qualifications are all good and how
others are all bad. This is just an honest attempt to provide an unbiased
approach towards these qualifications which might help an aspiring EM doctor!
I hope there will be less chaos in the days to
come and hope that the Governmental bodies and non-governmental professional
bodies work together instead of working against each other so that EM grows
further as a specialty in India. Hope there will be common ground of assessing
the competencies and logical conclusion to this without jeopardizing the
aspirations and dreams of people wanting to take up Emergency Medicine. In EM
we trust :)

Summary:
A. There are different ways of achieving
something. No one path is perfect for everyone. So what do you want to choose?
B. DO NOT believe people giving blanket
statements about things/issues. It's not just black or white!
C. Don't even believe this article. Do your
own critical appraisal!!!
D. Visit the college/hospital, speak to
residents/trainees, consultants before joining any program. Know what you are
doing and what you want to be!
E. Personally, depending upon all the above info,
I would rank the qualifications as follows:
1)DNB EM 1)MRCEM
2)MD EM 3) MEM
References:
Disclosures and Conflict of interest: I have done my 3 years EM residency from Apollo Hospitals Hyderabad and
have completed MRCEM. So there might be a slight positive bias towards Apollo
in the Article although a conscious effort has been made to avoid the same. The
views expressed here are the opinion of author only.
Author:

Dr. Apoorva Chandra
MBBS, MRCEM(UK)
Specialist Registrar – Emergency Medicine
Northwick Park Hospital
London, United Kingdom